Mental health awareness is growing — but confusion between PTSD and Complex PTSD remains widespread. Both are rooted in trauma, but they are distinct conditions with different origins, different impacts, and different roads to healing. Understanding the difference is not just clinical knowledge. For many people, it is the first time their experience has had a name.
📅 July 13, 2026 | ⏱ 11 min read | 🧠 Mental Health
- What Is Trauma? A Broader Understanding
- PTSD: When the Nervous System Gets Stuck
- Complex PTSD: When Trauma Rewires the Self
- Side by Side: The Key Differences
- Understanding “Disturbances in Self-Organisation”
- Trauma Lives in the Body
- Diagnosis and Recognition
- Treatment: Why the Path Looks Different
- Recovery Is Possible
- Frequently Asked Questions
You’ve heard of PTSD. You may have heard of Complex PTSD. Perhaps you’ve wondered whether one of them describes something you — or someone you love — have been living with, without ever having had the language for it.
The distinction between the two is not a matter of clinical technicality. For people who have been carrying one of these conditions — sometimes for decades, sometimes without a diagnosis, sometimes with the wrong one — understanding the difference can be quietly but profoundly validating. It can be the moment when a lifetime of confusing, painful, seemingly inexplicable experiences finally cohere into something that makes sense. Something that has a name. Something that, because it has been named, can be worked with.
Both PTSD and CPTSD are rooted in trauma. Both are real, serious, and treatable. And both deserve to be understood clearly — not lumped together, not minimised, and not misdiagnosed. This article gives you that understanding.

What Is Trauma? A Broader Understanding
Before distinguishing between PTSD and CPTSD, it helps to understand what trauma actually is — because the popular understanding of the word is significantly narrower than the clinical and neurological reality.
Trauma is not defined by the objective severity of an event. It is defined by the impact of that event on the nervous system. Trauma is what happens inside a person in response to an overwhelming experience — not simply the experience itself. Two people can live through the same event and be affected completely differently, depending on their neurobiology, their prior history, the presence or absence of support, their age, and dozens of other factors.
Peter Levine, one of the world’s leading trauma researchers, defines trauma as “any experience that overwhelms the nervous system’s capacity to cope” — leaving the threat response incompletely resolved, the nervous system frozen in a partial activation state that continues to fire as though the danger is ongoing.
Trauma can arise from:
- Single acute events — accidents, assaults, natural disasters, medical emergencies, witnessing violence
- Prolonged or repeated exposure — ongoing abuse, sustained neglect, domestic violence, war, captivity, trafficking
- Developmental trauma — early childhood experiences of unsafe, inconsistent, or frightening caregiving that shape the developing nervous system and attachment system
- Vicarious trauma — repeated exposure to others’ trauma (common in emergency services, healthcare, and social work)
- Collective and historical trauma — trauma transmitted across generations and communities through shared history of oppression, displacement, or violence
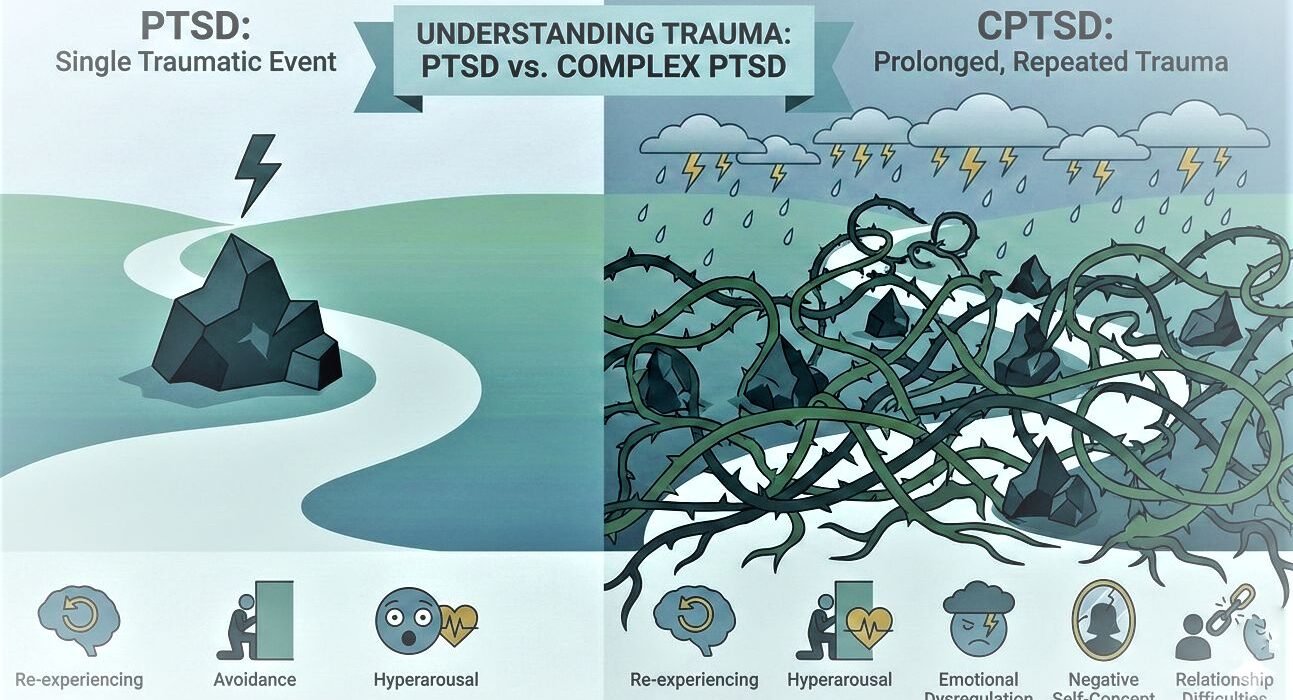
The distinction between PTSD and CPTSD maps most directly onto the first two categories — the difference between a single overwhelming event and prolonged, repeated, or developmental trauma. But as we’ll see, it is not only about duration. It is also about the relationship in which the trauma occurred, and the developmental stage at which it happened.
PTSD: When the Nervous System Gets Stuck
Post-Traumatic Stress Disorder is a well-established clinical diagnosis — recognised in the DSM-5 (the American diagnostic manual) and the ICD-11 (the international equivalent) — that develops in some people following exposure to a traumatic event or events.
The key word is “stuck.” The nervous system, which activated powerfully in response to threat, fails to return to a regulated baseline once the threat has passed. It remains in a state of high alert — responding to reminders of the trauma as though the original danger is still present. PTSD is, at its neurological core, a disorder of failed recovery from a traumatic event.
What Causes PTSD
PTSD is most strongly associated with single, acute, or time-limited traumatic experiences — though it can also develop from a series of discrete traumatic events. Common precipitants include:
- Serious road traffic accidents
- Natural disasters (earthquakes, floods, fires)
- Assault, rape, or sexual violence
- Witnessing death or serious injury
- Combat exposure
- Sudden traumatic bereavement
- Medical trauma (emergency surgery, life-threatening illness, traumatic childbirth)
Not everyone who experiences these events develops PTSD — research suggests that approximately 20–30% of people exposed to trauma go on to develop the condition, with women twice as likely as men to receive the diagnosis.
Core Symptoms of PTSD
| Symptom Cluster | What It Looks Like |
|---|---|
| Re-experiencing | Flashbacks — vivid, intrusive re-living of the traumatic event as though it is happening again in the present; nightmares; intense psychological or physical distress when reminded of the trauma |
| Avoidance | Deliberately avoiding thoughts, memories, people, places, activities, or situations associated with the traumatic event; emotional numbing or detachment as a protective mechanism |
| Hyperarousal | Persistent state of high alert — difficulty sleeping, irritability, difficulty concentrating, exaggerated startle response, hypervigilance (constantly scanning for danger) |
| Negative cognitions and mood | Persistent negative beliefs about oneself or the world (“I am permanently damaged,” “nowhere is safe”); persistent negative emotions; feelings of detachment from others; loss of interest in previously meaningful activities |
In PTSD, these symptoms are tied specifically to the traumatic event or events. The flashbacks replay that specific moment. The avoidance is of specific reminders. The hyperarousal was triggered by that specific threat. This specificity — the way symptoms orbit around a defined traumatic experience — is one of the features that distinguishes PTSD from CPTSD.
Complex PTSD: When Trauma Rewires the Self
Complex PTSD (CPTSD) was first described by psychiatrist Judith Herman in her landmark 1992 book Trauma and Recovery, in which she argued that the existing PTSD diagnosis was inadequate for capturing the experience of people who had endured prolonged, repeated, or developmental trauma — particularly trauma inflicted in the context of relationships of dependency and captivity, where escape was impossible or unthinkable.
After decades of advocacy by clinicians and researchers, CPTSD was formally recognised as a distinct diagnosis in the ICD-11 (the World Health Organization’s diagnostic manual) in 2019 — a significant milestone. It is not yet a separate diagnosis in the American DSM-5, which remains a point of ongoing clinical debate.
What Causes CPTSD
CPTSD arises from prolonged, repeated, or cumulative trauma — particularly trauma that is interpersonal in nature and occurs in situations where the person perceives no way to escape. The relational dimension is critical: this is not trauma inflicted by an impersonal force (a natural disaster, a car accident) but by other human beings, often those in positions of power, trust, or care.
Common contexts include:
- Long-term childhood abuse — physical, emotional, sexual, or neglect
- Sustained domestic violence
- Human trafficking and sexual exploitation
- Childhood in a chronically unsafe or unpredictable caregiving environment
- Refugee experiences and prolonged displacement
- Torture or prolonged captivity
- Long-term institutional abuse
- Cult membership and high-control group experiences
The developmental dimension matters enormously. When this type of trauma occurs during childhood — when the brain and attachment system are still forming — its impact is qualitatively different from trauma experienced in adulthood. It doesn’t only affect how the person responds to danger. It shapes how they experience themselves, other people, their own emotions, and the world.
Core Symptoms of CPTSD
CPTSD includes all the core symptoms of PTSD — re-experiencing, avoidance, and hyperarousal — and adds a further cluster of symptoms that reflect the deeper, self-level impact of prolonged relational trauma. These additional symptoms are called Disturbances in Self-Organisation (DSO) and represent what makes CPTSD distinct:
| Disturbance | What It Looks Like |
|---|---|
| Severe emotional dysregulation | Intense, rapidly shifting emotional states that feel overwhelming and hard to manage; emotional reactions that feel disproportionate to the trigger; difficulty returning to baseline after being upset; emotional numbness or dissociation at other times |
| Pervasive negative self-concept | A deep, often shame-based sense of being fundamentally different from other people — permanently broken, damaged, worthless, or defective. Not a belief about a specific event, but a belief about the self at its core. Often accompanied by profound shame and self-loathing. |
| Difficulties in relationships | Chronic difficulty trusting others; oscillating between intense attachment and sudden withdrawal; difficulty maintaining relationships over time; either avoiding intimacy entirely or becoming enmeshed; hypervigilance about others’ motives and potential for betrayal |
Side by Side: The Key Differences
| Factor | PTSD | Complex PTSD (CPTSD) |
|---|---|---|
| Trauma type | Single, acute, or time-limited traumatic event(s) | Prolonged, repeated, cumulative trauma — often interpersonal, often developmental |
| Duration | Short-term or episodic trauma | Months or years of repeated or ongoing trauma |
| Relationship to perpetrator | Often impersonal or stranger-involved; not necessarily relational | Typically relational — perpetrated by a caregiver, partner, or authority figure; trust was involved |
| Core symptoms | Re-experiencing, avoidance, hyperarousal, negative cognitions | All PTSD symptoms PLUS emotional dysregulation, negative self-concept, relationship difficulties |
| Focus of symptoms | Tied specifically to the traumatic event — re-living, avoiding, being triggered by reminders of that event | Pervasive — affects identity, self-worth, relationships, emotional life, and worldview broadly |
| Self-concept | May include negative beliefs about the specific event (“I should have done something”), but core identity is typically intact | Core identity is significantly affected — profound shame, sense of being permanently damaged or defective, fundamental self-loathing |
| Relationships | May be affected, particularly if the trauma was interpersonal, but relationship capacity is largely intact | Chronic and pervasive difficulty trusting, maintaining intimacy, and sustaining stable relationships |
| Developmental impact | Less common in purely developmental trauma; more often adult-onset | Frequently rooted in childhood and developmental trauma; the developing brain and attachment system are directly shaped |
Understanding “Disturbances in Self-Organisation”
The term “disturbances in self-organisation” — the defining additional cluster of CPTSD — can sound abstract. But for people living with it, these disturbances are anything but abstract. They are the daily texture of a life shaped by prolonged relational trauma, and understanding them specifically matters enormously for both self-recognition and treatment.
Emotional Dysregulation
People with CPTSD often describe their emotional life as being controlled by something outside themselves. Emotions arrive with overwhelming intensity — terror, rage, shame, despair — and are extremely difficult to de-escalate once activated. The emotional response system, shaped by years of chronic threat, is sensitised to interpersonal cues that register (accurately, based on past experience) as dangerous: a change in someone’s tone, a perceived withdrawal, an ambiguous message.
At other times, the opposite occurs: emotional numbness, flatness, dissociation — a shutting down of feeling as a protective mechanism that became habitual under conditions of inescapable threat. Many people with CPTSD oscillate between these two states: floods of unbearable feeling and complete emotional disconnection.
Pervasive Negative Self-Concept
This is perhaps the most painful — and most misunderstood — dimension of CPTSD. It is not a belief about a specific event (“I feel guilty about what happened”). It is a belief about the self at its foundation: I am broken. I am damaged beyond repair. I am fundamentally different from normal people. Something is permanently wrong with me. I am unlovable, unworthy, contaminated.
This self-concept is not irrational or evidence of cognitive distortion, though it may be addressed through cognitive means. It is the logical conclusion of years of being treated as though you didn’t matter, weren’t safe, or deserved harm — particularly when that treatment came from the people who were supposed to love and protect you. The child who is repeatedly abused or neglected by a caregiver has two options: believe the caregiver is unsafe, or believe they themselves are the problem. The second option is developmentally more bearable — and it hardens into a core belief that persists long after the original circumstances are gone.
Difficulties in Relationships
When trauma is relational — when the people who hurt you were the people you needed, depended on, or loved — the attachment system is fundamentally disrupted. Safety and threat become neurologically entangled. Closeness becomes associated with danger. Trust becomes almost impossible to extend fully, because the history says trust leads to betrayal.
The result, in adult relationships, is often a painful paradox: desperately wanting connection while being terrified of it. Pushing people away or withdrawing before the anticipated abandonment arrives. Scanning relationships constantly for signs of threat. Difficulty believing that care is genuine or that it will last. And sometimes, a gravitational pull toward relationships that replicate the familiar pattern of harm — because the nervous system has been calibrated to the landscape of danger.
🔬 Important Note: Many people with CPTSD have spent years — sometimes decades — being misdiagnosed with borderline personality disorder, bipolar disorder, depression, anxiety, or ADHD. While these conditions can co-occur with CPTSD, the confusion arises because the symptoms of CPTSD (emotional dysregulation, unstable sense of self, relationship difficulties) overlap with several other diagnoses. An accurate trauma-informed assessment is essential for appropriate treatment. If your history includes prolonged relational trauma and previous diagnoses haven’t fully explained or addressed your experience, it may be worth exploring CPTSD with a trauma-informed clinician.
Trauma Lives in the Body
One of the most important insights of modern trauma research — advanced particularly by Bessel van der Kolk’s landmark work — is captured in the title of his book: The Body Keeps the Score.
Trauma is not only a memory. It is not only a thought pattern. It is a physiological state — encoded in the nervous system, the musculature, the hormonal system, and the body’s threat-response architecture. This is why talking about trauma, while valuable, is rarely sufficient on its own for full recovery. The nervous system needs to be directly addressed — to complete the cycles of activation that were interrupted or frozen by the original trauma.
Both PTSD and CPTSD manifest in the body in specific, recognisable ways:
| Body System | How Trauma Shows Up |
|---|---|
| Autonomic nervous system | Chronic sympathetic activation (fight/flight) or dorsal vagal shutdown (freeze/collapse); difficulty finding and staying in a regulated, calm state |
| HPA axis (stress hormones) | Dysregulated cortisol patterns — either chronically elevated or blunted (a sign of long-term exhaustion of the stress response system) |
| Musculoskeletal system | Chronic muscle tension, particularly in the jaw, neck, shoulders, hips, and pelvic floor; unexplained pain; the body holding the bracing response of unresolved threat |
| Digestive system | IBS-like symptoms, chronic digestive disturbance, nausea; the gut-brain axis carries the imprint of prolonged stress |
| Brain structure | Research has documented measurable changes in the amygdala (enlarged, hyperreactive), hippocampus (reduced volume, affecting memory integration), and prefrontal cortex (reduced activity, affecting regulation) in people with trauma histories |
Diagnosis and Recognition
PTSD is recognised in both the DSM-5 and ICD-11. CPTSD is recognised in the ICD-11 but not yet as a separate diagnosis in the DSM-5 — a gap that has significant clinical implications, particularly in the United States, where DSM classification affects insurance coverage and treatment access.
In practice, this means that people with CPTSD may be diagnosed under PTSD, or may receive diagnoses of personality disorder, depression, or anxiety that don’t fully capture their experience. Receiving an accurate diagnosis — ideally from a trauma-informed clinician who is familiar with CPTSD — is an important step. Not because labels define us, but because the right label points toward the right treatment, the right framework, and crucially: validation that your experience is real, has a name, and can be worked with.
If you are working through whether CPTSD might describe your experience, a few questions worth sitting with:
- Does your history include prolonged, repeated, or developmental trauma — particularly in the context of relationships?
- Do you experience your emotional reactions as disproportionate, overwhelming, or very difficult to regulate?
- Do you carry a pervasive sense of shame — not just about specific things, but about yourself as a person?
- Do you find close relationships chronically difficult — marked by fear of abandonment, difficulty trusting, or painful oscillations between closeness and withdrawal?
- Do you feel fundamentally different from others — as though they have access to something basic about functioning in the world that you have never had?
If these questions resonate, a trauma-informed therapist or psychiatrist is the appropriate next step.
Treatment: Why the Path Looks Different
Because PTSD and CPTSD have different structures — PTSD organised around specific traumatic memories, CPTSD organised around a disrupted sense of self and chronic dysregulation — their treatment approaches, while overlapping, are importantly different.
Treating PTSD
For PTSD, evidence-based first-line treatments focus on processing the specific traumatic memory to reduce its emotional charge and integrate it into the broader narrative of the person’s life:
- EMDR (Eye Movement Desensitisation and Reprocessing) — one of the most strongly evidenced treatments for PTSD; processes traumatic memories through bilateral stimulation
- Prolonged Exposure Therapy — gradually and systematically confronting trauma reminders to reduce avoidance and desensitise the fear response
- Trauma-focused CBT (TF-CBT) — addressing trauma-related thought patterns alongside graduated exposure to trauma memories
- Cognitive Processing Therapy (CPT) — specifically targeting the “stuck points” — distorted beliefs about the self and world that develop after trauma
Treating CPTSD
For CPTSD, treatment is generally more complex, longer-term, and phased. Jumping directly into trauma processing without first building sufficient safety, stabilisation, and emotional regulation capacity can be destabilising or re-traumatising. The widely accepted phased approach involves:
| Phase | Focus | What It Involves |
|---|---|---|
| Phase 1: Safety and Stabilisation | Building the foundation for healing | Establishing physical and psychological safety; developing emotional regulation skills; building distress tolerance; creating a stable therapeutic relationship |
| Phase 2: Trauma Processing | Working through the trauma itself | Graduated processing of traumatic memories and their meaning; approaches may include EMDR, somatic therapy, schema therapy, or parts-based approaches |
| Phase 3: Integration and Reconnection | Building the life after trauma | Integrating the processed experiences into a coherent life narrative; rebuilding identity and self-concept; developing healthy relationships; engaging with life and meaning |
Additional approaches with particular relevance to CPTSD include:
- Schema therapy — addressing the core early maladaptive schemas (deeply held beliefs about self and relationships) that develop from developmental trauma
- Internal Family Systems (IFS) — a parts-based approach that works with the different “parts” of the self that developed as protective responses to trauma
- Somatic approaches — body-based therapies including Somatic Experiencing, Sensorimotor Psychotherapy, and trauma-sensitive yoga, which address the physiological dimension of trauma directly
- Compassion-Focused Therapy (CFT) — particularly well-suited to the shame and self-loathing that characterise the negative self-concept of CPTSD
Recovery Is Possible
This must be said clearly, without qualification or hedging: recovery from both PTSD and CPTSD is entirely possible. Not just management. Not just coping. Genuine, meaningful recovery — a life in which the trauma no longer controls how you feel, how you function, and who you believe yourself to be.
Recovery from CPTSD is often a longer and more complex journey than recovery from single-event PTSD — because the work involves not just processing specific traumatic memories, but rebuilding a sense of self that was shaped from the beginning by harm. That is profound work. It takes time, skilled support, and enormous courage.
But people do it. Every day, people who have lived through unimaginable things — who were told, explicitly or implicitly, that they were beyond repair — find their way to lives that are genuinely their own. Lives where relationships feel possible. Where the body feels like home. Where the shame that once felt like identity begins to loosen, and something else — something truer — emerges in its place.
Whether your trauma was a single moment or a lifetime of moments —
you are not the sum of what happened to you. You are not permanently broken. You are a person who experienced something that overwhelmed their system — and whose system responded in the only ways it knew how to survive. That survival was intelligence, not weakness. And healing is available to you.
✦ Key Takeaways
- PTSD develops from single, acute, or time-limited traumatic events and is characterised by re-experiencing, avoidance, and hyperarousal tied specifically to that event.
- CPTSD develops from prolonged, repeated, or developmental trauma — especially interpersonal trauma in situations of captivity or dependency — and includes all PTSD symptoms plus disturbances in self-organisation.
- The three disturbances in self-organisation that define CPTSD are: severe emotional dysregulation, a pervasive negative self-concept rooted in shame, and chronic difficulties in trusting and maintaining relationships.
- CPTSD is recognised in the ICD-11 (World Health Organization) as a distinct diagnosis. Misdiagnosis as borderline personality disorder, bipolar disorder, or depression is common — an accurate trauma-informed assessment matters.
- Treatment for PTSD focuses on processing specific traumatic memories. Treatment for CPTSD is phased — establishing safety and stabilisation before trauma processing — and is generally longer-term and more complex.
- Recovery from both conditions is entirely possible with trauma-informed care. You are not permanently broken. Healing is available to you.
Frequently Asked Questions
Can you have both PTSD and CPTSD?
The ICD-11 treats CPTSD as a distinct condition that includes PTSD symptoms — so technically, a diagnosis of CPTSD already encompasses the PTSD symptom cluster. However, someone with a background of complex developmental trauma may also experience a later single-event trauma that exacerbates or reactivates symptoms. In clinical practice, the treatment approach would address both the complex, developmental dimensions and any specific traumatic events that require direct processing. If you have a history of both, a thorough trauma-informed assessment will help determine the most appropriate treatment pathway.
How is CPTSD different from borderline personality disorder?
This is one of the most clinically important questions in trauma psychiatry. CPTSD and BPD share several surface features — emotional dysregulation, relationship difficulties, unstable sense of self — which has led to significant misdiagnosis of CPTSD as BPD. The key differences are: CPTSD is understood as a response to external trauma (the disorder lies in what happened), while BPD has historically been framed as a more constitutional personality structure (though trauma is implicated in BPD as well); CPTSD does not include the impulsivity, identity diffusion, or fear of abandonment-driven reactive behaviours that are specific to BPD; and crucially, many advocates argue that BPD itself may largely represent unrecognised CPTSD. This remains an active area of clinical debate. What is clear is that an accurate, trauma-informed assessment by a clinician familiar with both conditions is essential before either label is applied.
Can CPTSD develop in adulthood — not just childhood?
Yes — absolutely. While developmental trauma (particularly in childhood and adolescence) creates a particular depth of impact because the brain and attachment system are still forming, CPTSD can develop from prolonged relational trauma experienced at any age. Adults in sustained domestic violence situations, people held in captivity, survivors of prolonged workplace abuse, and those in high-control groups or cults can all develop CPTSD even if their early childhood was largely stable. The key factors are not age alone but duration, the relational quality of the trauma, and the perceived impossibility of escape.
Is medication helpful for PTSD and CPTSD?
Medication can play a supportive role, particularly in the early stages of treatment when symptoms are most overwhelming. SSRIs (particularly sertraline and paroxetine) are the most commonly prescribed medications for PTSD — they are approved for this use and have a reasonable evidence base for reducing symptom severity. Prazosin has evidence for reducing trauma-related nightmares. For CPTSD, medication is generally considered a support rather than a primary treatment — the core disturbances in self-organisation are not fundamentally pharmacological in nature. Most trauma specialists recommend medication as an adjunct to therapy rather than a standalone intervention, and any medication decisions should be made in consultation with a psychiatrist or informed prescriber.
What should I do if I think I have CPTSD?
The most important first step is to seek an assessment from a trauma-informed clinician — ideally one who is specifically familiar with CPTSD as a distinct diagnosis. A GP can provide a referral, or you may be able to access a trauma-specialist therapist or psychiatrist directly. When looking for a therapist, it is worth specifically asking about their experience with complex trauma, CPTSD, and the phased treatment approach. Not all therapists are equally trained in this area, and for complex trauma in particular, the right match and the right expertise genuinely matter. If cost or access is a barrier, trauma-informed community mental health services, sliding-scale therapists, and peer support organisations for trauma survivors are all worth exploring.
If you are living with trauma and would like to speak with someone, please reach out to a trauma-informed mental health service or crisis line in your country. You deserve support, and help is available.
Evidence-based wellness content to help you feel your best — body and mind. | The Whole You Wellness


Leave a Comment