One of the most hopeful ideas in therapy is also one of the simplest: your thoughts, feelings, and actions are all connected — which means change in one area can gently shift the others. This article unpacks how that works, and how you can use it.
📅 August 17, 2026 | ⏱ 9 min read | 🧠 Mental Health
- What Is CBT?
- The CBT Triangle Explained
- Thoughts: The Stories We Tell Ourselves
- Feelings: The Body Keeping Score
- Actions: The Behaviours That Keep Cycles Alive
- Common Cognitive Distortions
- Breaking the Cycle — Entry Points for Change
- CBT in Practice: What It Actually Looks Like
- A Note on Self-Compassion
- Frequently Asked Questions
You wake up and immediately think: today is going to be hard. That thought sits in your chest, and the feeling that follows — low, heavy, already a little defeated — makes you want to stay in bed. And staying in bed confirms, by the end of the day, that you were right: it was hard. The thought shaped the feeling that shaped the behaviour that confirmed the thought.
This is not a moral failing. It is a loop — one that most of us cycle through dozens of times each day without realising it. And it is exactly what Cognitive Behavioural Therapy (CBT) was built to address: not by judging the loop, not by demanding you think positive thoughts, but by helping you notice the loop, understand how it works, and find the leverage points where gentle, consistent change becomes possible.
The most hopeful thing about the CBT model is its bidirectionality. Thoughts affect feelings affect actions — but the relationship runs in every direction. Which means you don’t have to fix your thinking before you can feel better, and you don’t have to feel better before you can act differently. Change can begin anywhere in the triangle, and ripple outward.

What Is CBT?
Cognitive Behavioural Therapy is one of the most extensively researched psychological treatments in existence, with a robust evidence base across anxiety disorders, depression, OCD, eating disorders, chronic pain, PTSD, insomnia, and many other conditions. Developed primarily by Aaron Beck in the 1960s (from roots in Albert Ellis’s Rational Emotive Behaviour Therapy), CBT is based on the fundamental insight that psychological distress is maintained not just by circumstances — by what happens to us — but by the meaning we assign to what happens, and the ways we respond to it.
The model is pragmatic, collaborative, and skills-based. It gives people concrete tools they can use in real life, not just in the therapy room. It works on the principle that — with support, practice, and self-compassion — most people can learn to recognise and modify the patterns of thought and behaviour that maintain their distress.
🔬 The Evidence: A meta-analysis of over 400 studies found CBT to be effective for a broad range of presentations, with effect sizes comparable to or exceeding medication for many anxiety and depressive conditions — and with more durable effects, since the skills learned in CBT continue to be available after treatment ends in a way that medication alone does not provide.
The CBT Triangle Explained
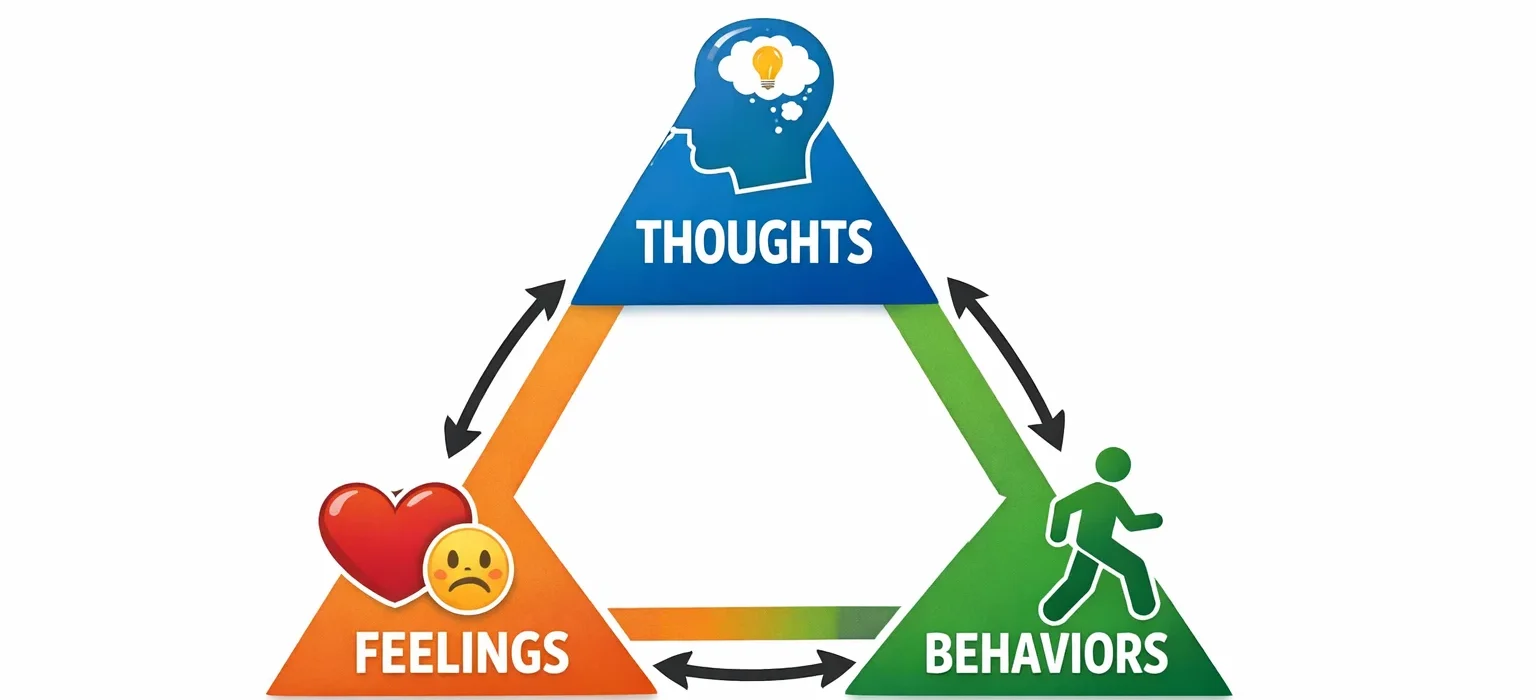
At the heart of CBT is a simple but powerful model: the cognitive triangle (sometimes called the CBT triangle). It describes the relationship between three elements of experience that are continuously influencing one another:
💭 THOUGHTS
What we think affects how we feel & act
interconnected
↑
🏃 ACTIONS
What we do affects how we think & feel
💛 FEELINGS
What we feel affects how we act & think
Each element influences the others — in every direction
The arrows in the triangle run in every direction — and this is the crucial point. The relationship between thoughts, feelings, and actions is not a one-way street. Each element continuously influences the others, creating either a downward spiral (when the cycle is negative) or an upward one (when the cycle is positive).
The classic example from your infographic captures this perfectly:
Thought: “No one likes me.” →
Feeling: Sadness, disconnection. →
Action: Stay in bed, avoid others. →
New thought: “See — I’m alone. I knew no one liked me.”
The cycle feeds itself — and the loop continues until something interrupts it.
Notice how the action of staying in bed doesn’t just follow from the thought and feeling — it confirms the original thought by providing evidence for it. The person stays in bed, has fewer positive social interactions, and the thought “no one likes me” is reinforced. This is why breaking unhelpful cycles often requires more than just changing how you think. It requires understanding the full loop — and finding where you can introduce a different response.
Thoughts: The Stories We Tell Ourselves 💭
In the CBT model, “thoughts” doesn’t refer only to the deliberate, conscious reflections you have when you sit down to think about something. It refers primarily to automatic thoughts — the rapid, often unconscious interpretations and evaluations that flow through the mind constantly in response to events, sensations, and situations.
Automatic thoughts are fast, involuntary, and often feel like facts rather than interpretations. “That was embarrassing” doesn’t usually arrive as a tentative hypothesis — it arrives as a statement of obvious reality. The emotional response that follows reinforces its felt truth. And yet automatic thoughts — like all thoughts — are interpretations, shaped by our history, our beliefs about ourselves and the world, and the cognitive patterns we’ve developed over time.
These patterns, in CBT, sit on top of deeper structures:
| Level | What It Is | Example |
|---|---|---|
| Automatic thoughts | Fast, surface-level interpretations triggered by specific situations | “I made a mistake in that presentation — everyone thinks I’m incompetent.” |
| Intermediate beliefs | Rules and assumptions that generate automatic thoughts: “If I make a mistake, people will judge me.” “I should always perform perfectly.” | “If I’m not perfect, I am worthless.” |
| Core beliefs | Deep, global beliefs about the self, others, and the world — formed early, felt as absolute truth | “I am fundamentally inadequate.” “The world is a dangerous place.” “I am unlovable.” |
Standard CBT primarily works at the level of automatic thoughts — the most accessible and most directly modifiable layer. Deeper work on intermediate and core beliefs often occurs in longer-term therapy, including schema therapy or psychodynamic approaches. But even at the surface level of automatic thoughts, meaningful change is possible — and the ripple effects on feelings and behaviour can be significant.
Feelings: The Body Keeping Score 💛
In the CBT triangle, “feelings” refers to emotions — but also to the physical sensations that always accompany them. Emotions are not purely mental events. They are embodied experiences: the tight chest of anxiety, the heaviness of depression, the heat of shame, the restlessness of frustration. These physical dimensions are part of the feeling, not separate from it.
In CBT’s original formulation, feelings were understood primarily as consequences of thoughts — emotions follow from the meanings we assign to events. And this is true: the interpretation shapes the emotional response. Two people can experience the same event (being passed over for a promotion) and feel very different things depending on the story they tell about it (“I’m not good enough” vs “this company doesn’t value what I bring”).
But the relationship is also reciprocal. Feelings influence thoughts — the way a low mood makes negative interpretations more available and more convincing, or the way anxiety narrows the mind’s field of possibilities. This bidirectionality is why directly targeting the feeling — through breathing, movement, body-based practices — can shift the cognitive landscape without any deliberate cognitive work at all.
An important nuance: in CBT, the goal is not to eliminate negative feelings or always feel good. Difficult emotions — sadness, fear, anger, grief — are appropriate responses to genuinely difficult circumstances. The goal is to reduce the suffering that comes from emotions that are disproportionate to the situation, that persist longer than necessary, or that are amplified by the cognitive layer on top of them.
Actions: The Behaviours That Keep Cycles Alive 🏃
The “actions” corner of the triangle refers to behaviour — what we do in response to our thoughts and feelings. In CBT, behaviour is as important as cognition, because behaviour maintains cycles in ways that thought alone cannot change.
The two most clinically significant behavioural patterns in maintaining psychological distress are:
Avoidance
Avoiding situations, people, sensations, or thoughts associated with distress produces immediate relief — which neurologically reinforces the avoidance. But it also prevents the learning that could reduce the distress: the discovery that the feared situation was manageable, that the dreaded outcome didn’t occur, that you have more capacity to cope than you believed. Avoidance relieves anxiety in the moment and maintains it long-term. This is why behavioural activation and exposure-based approaches are central to CBT for anxiety and depression.
Safety behaviours
Subtler than avoidance, safety behaviours are the things we do in feared situations to prevent the feared outcome — sitting near the exit in social situations, checking repeatedly that the door is locked, over-preparing to prevent catastrophic performance. While they reduce immediate anxiety, safety behaviours prevent the disconfirmation of the feared belief. The person who sat near the exit will attribute their survival of the social event to the exit, not to evidence that they could have coped — and the belief that they couldn’t cope remains intact.
This is one of the reasons that changing behaviour — particularly approaching rather than avoiding what we fear — is one of the most powerful interventions available. Action has the unique capacity to provide evidence that thought alone cannot generate.

Common Cognitive Distortions
A core component of CBT is learning to recognise “cognitive distortions” — systematic errors in thinking that make interpretations more negative, more extreme, or more global than the evidence warrants. These are not signs of stupidity or irrationality. They are patterns that develop, often in childhood, as ways of making sense of a world that felt difficult — and that persist into adulthood, colouring experience in ways we often don’t notice.
| Distortion | What It Is | Example |
|---|---|---|
| All-or-nothing thinking | Seeing things in black and white — no middle ground, no nuance, no “good enough” | “If it’s not perfect, it’s a complete failure.” |
| Catastrophising | Assuming the worst possible outcome will occur; amplifying the significance of difficulties | “I made one mistake at work — I’m going to be fired.” |
| Mind reading | Assuming you know what others are thinking — usually negatively about you | “They didn’t reply — they must be angry with me.” |
| Overgeneralisation | Drawing sweeping conclusions from a single event — always, never, everyone, no one | “I failed this — I always fail at everything.” |
| Personalisation | Taking excessive responsibility for events outside your control; assuming everything is about you | “They seem upset — it must be something I did.” |
| Emotional reasoning | Treating feelings as facts — because I feel it, it must be true | “I feel stupid, therefore I am stupid.” |
| Filtering | Focusing exclusively on the negative aspects of a situation while filtering out the positive | Receiving nine positive pieces of feedback and one criticism — and only thinking about the criticism. |
| “Should” statements | Rigid rules about how you or others must behave — creating guilt when violated | “I should be able to handle this. I shouldn’t need help.” |
Recognising a cognitive distortion does not make it disappear. But naming it — “that’s all-or-nothing thinking happening” — creates a small but significant distance between you and the thought. It introduces the possibility that the thought is a pattern, not a fact. And that possibility is the crack through which change enters.
Breaking the Cycle — Entry Points for Change
Because the triangle runs in every direction, there are multiple entry points for change. You don’t have to start with thoughts. You don’t have to feel better before you act. Change can begin anywhere — and the choice of entry point can be made based on what is most accessible to you in your current state.
💭
Entering through thoughts
Noticing automatic thoughts, examining the evidence for and against them, and developing more balanced alternatives. Best when the emotional intensity is moderate — not so high that cognitive work is impossible, not so low that there’s nothing to work with.
💛
Entering through feelings
Directly regulating the emotional and physiological state — through breathing, movement, grounding, or sensory activation — to reduce the intensity that makes cognitive work difficult. Particularly useful when emotional flooding is high.
🏃
Entering through actions
Changing behaviour first — approaching what you’ve been avoiding, activating rather than withdrawing, doing something that generates evidence against a negative belief. Particularly useful in depression, where motivation and cognitive capacity are both compromised.
In practice, most effective CBT work uses all three entry points — moving between them depending on what the moment calls for. The triangle is not a rigid hierarchy. It is a map of a dynamic system, and the skilled use of it is knowing where the leverage is at any given moment.
CBT in Practice: What It Actually Looks Like
CBT is one of the most structured and skills-based therapies available — which means it looks quite different from the popular image of therapy as open-ended talking. A CBT therapist and client work collaboratively, with a clear shared understanding of the presenting problem and the goals of treatment. Sessions are typically focused, with an agenda, and include homework — not as a burden, but as the bridge between the therapy room and the actual life in which change needs to happen.
Thought records
One of the most commonly used CBT tools is the thought record — a structured written exercise that helps identify automatic thoughts in specific situations, examine the evidence for and against them, and develop a more balanced alternative thought. Used consistently, thought records build the habit of cognitive flexibility: the ability to notice a thought and ask “is this actually true?” rather than accepting it as reality.
Behavioural experiments
Rather than arguing with a belief in the abstract, behavioural experiments test it in real life. If the belief is “I can’t cope in social situations,” the experiment might involve attending a specific social event and observing what actually happens — not what was predicted. The lived evidence generated by experiments is typically far more persuasive than any amount of reasoning. The body learns differently from the mind. It learns through experience.
Graded exposure
For anxiety-maintaining avoidance, CBT uses graduated exposure — approaching feared situations in a systematic, stepwise way, starting with the least feared and building toward the most feared. Each successful step disconfirms the predicted catastrophe and builds evidence of coping capacity. Over time, the feared stimulus loses its power — not because the danger is argued away, but because the nervous system learns through repeated experience that it is manageable.
Behavioural activation
For depression, where withdrawal and inactivity maintain low mood, behavioural activation involves scheduling and completing activities that generate a sense of pleasure or achievement — even when motivation is absent. The key insight is counterintuitive: in depression, action precedes motivation, not the other way around. You don’t wait to feel like doing things. You do things, and the feeling gradually follows.
A Note on Self-Compassion
A common misunderstanding of CBT is that it involves judging yourself for unhelpful thoughts — catching yourself thinking “negatively” and correcting it, as if unhelpful thoughts were mistakes to be stamped out. This is not what good CBT involves. And it is worth saying clearly, because the self-critical application of a tool designed to reduce self-criticism would be its own kind of trap.
Many of us developed these patterns — the catastrophising, the worst-case thinking, the constant vigilance for threat — because they genuinely helped us survive difficult circumstances. They are not failures of character. They are adaptations. They made sense when they were formed. The CBT triangle is a map for understanding patterns with curiosity, not a weapon for judging yourself for having them.
The most effective CBT is delivered — and practised — in a spirit of compassionate curiosity: “I notice I’m doing that pattern again. That’s interesting. What might a more accurate or balanced perspective look like?” Not “I’m doing it wrong again.” The goal is not to think correctly. It is to think more flexibly — to hold your interpretations as possibilities rather than as facts, and to build a more spacious relationship with the full range of your mental and emotional experience.
“With practice, noticing automatic thoughts and experimenting with kinder, more balanced alternatives — without judging yourself for having them — can ease anxiety, soften self-criticism, and build everyday resilience.”
✦ Key Takeaways
- The CBT triangle describes the continuous, bidirectional relationship between thoughts, feelings, and actions — each one influencing the others in a cycle that can be either self-reinforcing or self-correcting.
- Thoughts affect feelings affect actions — but change can begin anywhere in the triangle. You don’t have to fix your thinking first, feel better first, or wait for motivation before acting differently.
- Automatic thoughts are fast, involuntary interpretations that feel like facts. They sit on top of deeper intermediate beliefs and core beliefs — and with practice, can be noticed, examined, and reframed.
- Avoidance and safety behaviours are among the most powerful maintainers of distress — because they prevent the lived experience that would disconfirm feared beliefs. Approaching rather than avoiding is one of the most powerful interventions available.
- Cognitive distortions — all-or-nothing thinking, catastrophising, emotional reasoning, and others — are not signs of irrationality. They are patterns, often formed in difficult circumstances, that can be recognised and gently challenged.
- CBT works best in a spirit of self-compassion — curious about patterns, not judgemental of them. The goal is more flexible, more accurate, and kinder thinking — not perfect thinking.
Frequently Asked Questions
How is CBT different from positive thinking?
This is one of the most important distinctions to make — because CBT is frequently and inaccurately characterised as “just think positive.” It is not. CBT does not ask you to replace negative thoughts with positive ones, deny difficult realities, or force optimism. It asks you to examine whether your current interpretation of events is accurate — to check the evidence — and to develop thoughts that are realistic and balanced rather than either unrealistically negative or unrealistically positive. “Balanced” is the goal, not “positive.” A CBT therapist might ask: “What is the evidence for this thought? What is the evidence against it? What might a more accurate, complete picture look like?” The answer is often neither as catastrophic as the original thought nor as rosy as forced positivity.
Can I do CBT by myself without a therapist?
Self-directed CBT — through workbooks, apps, and structured online programmes — has a reasonable evidence base for mild to moderate anxiety and depression. For many people, learning and applying CBT skills independently produces meaningful benefit. However, self-directed CBT has limitations: it is harder to identify your own cognitive distortions than to identify someone else’s, the motivational and relational dimensions of working with a skilled therapist are not replicable alone, and for more complex or severe presentations, professional support is important. Self-directed CBT tools are best used as a complement to professional support, as a starting point before accessing therapy, or as a maintenance tool after therapy has built the foundational skills.
How long does CBT take to work?
CBT is one of the shorter-term evidence-based therapies — typically delivered over 8 to 20 sessions for most presentations. For focused, specific issues (a specific phobia, mild panic disorder) even fewer sessions may be sufficient. For more complex presentations, or where the work extends to deeper intermediate and core beliefs, longer-term work is appropriate. Most people notice some meaningful shift — in their relationship to their thoughts and in the intensity of associated feelings — within the first several sessions, though sustained change typically requires consistent practice between sessions and over time.
Is CBT suitable for trauma?
Trauma-focused CBT (TF-CBT) is a specifically adapted protocol with strong evidence for PTSD — including in both children and adults. It includes the standard CBT components alongside specific trauma processing elements (exposure to the trauma memory and reprocessing of its meaning). For complex trauma (CPTSD), standard CBT is typically insufficient — the stabilisation and emotional regulation work that must precede trauma processing requires a phased approach, and approaches including EMDR, somatic therapy, and schema therapy are often integrated. A trauma-informed therapist can assess which approach is most appropriate for a specific trauma history and presentation.
What if I’ve tried CBT and it didn’t help?
CBT is not effective for everyone, and this is important to acknowledge honestly. Several factors affect outcomes: the quality of the therapeutic relationship, whether the CBT was delivered with fidelity to the model, whether the presenting issue was well-matched to a CBT approach, and whether any underlying factors (trauma, neurobiological vulnerability, medication need) were addressed. If CBT hasn’t helped, it is worth exploring: was it full CBT with a trained therapist, or a brief or low-intensity version? Was there a good therapeutic relationship? Is there a trauma history that may require a different primary approach? Other evidence-based approaches — ACT, DBT, schema therapy, EMDR, psychodynamic therapy — may be a better fit for certain presentations and certain people. No single approach works for everyone, and the absence of benefit from one approach is not a sign that benefit from another is unavailable.

If you’d like to explore CBT with a trained therapist, ask your GP for a referral or search for a CBT-accredited practitioner in your area. You deserve support — and this is one of the most effective tools available for building a healthier, more flexible relationship with your own mind.
Evidence-based wellness content to help you feel your best — body and mind. | The Whole You Wellness

Leave a Comment