
You know the relationship is hurting you. You’ve seen the pattern dozens of times. And yet leaving feels impossible — and staying feels like love. This is trauma bonding: one of the most misunderstood and least talked about psychological experiences a person can have.
📅 June 15, 2026 | ⏱ 11 min read | 🧠 Mental Health
- What Is Trauma Bonding?
- How Trauma Bonds Form: The Cycle
- The Childhood Roots of Trauma Bonding
- The Neuroscience: Why Your Brain Stays
- Signs You May Be Trauma Bonded
- Where Trauma Bonding Happens
- Trauma Bonding Is Not Weakness
- Healing From a Trauma Bond
- What Healthy Love Actually Feels Like
- Frequently Asked Questions
There is a particular kind of confusion that comes with being in a harmful relationship — not the confusion of not knowing what’s happening, but the deeper confusion of knowing and still not being able to leave. Of loving someone who hurts you. Of missing them even while you’re still with them. Of defending them to others when part of you knows the truth.
This is not weakness. This is not stupidity. This is not a lack of self-respect. This is trauma bonding — a well-documented psychological and neurological phenomenon that happens when a powerful emotional attachment forms inside a cycle of harm and intermittent kindness.
Trauma bonding affects people across every demographic, every level of education, every type of relationship. It is found in romantic partnerships, parent-child relationships, friendships, cults, and workplaces. It has been studied in prisoners of war, hostages, and abuse survivors. And it is, at its core, not a sign of something broken in the person experiencing it — it is a sign of a nervous system doing exactly what nervous systems evolved to do in conditions of threat and unpredictable affection.
Understanding trauma bonding — what it is, how it forms, why it feels the way it does, and how to begin healing from it — is some of the most important psychological knowledge a person can have. This article gives you that understanding.
What Is Trauma Bonding?
Trauma bonding is a deep emotional attachment that forms between a person and someone who repeatedly causes them harm. It is characterised by a powerful, often overwhelming sense of connection, loyalty, and love toward someone whose behaviour is inconsistent, manipulative, or abusive — and by extreme difficulty breaking that attachment even when the person is fully aware it is harmful.
The term was first developed by psychologist Patrick Carnes, who used it to describe the emotional bonds that form in relationships characterised by a power imbalance, intermittent abuse, and cycles of punishment and reward. It has since been extensively studied across multiple contexts — from intimate partner violence to child maltreatment, from hostage situations (where it was first observed as “Stockholm Syndrome”) to cult membership.
What makes trauma bonding distinctively painful — and distinctively confusing — is that the bond does not feel like the result of harm. It feels like love. It feels like a connection deeper than any you’ve known. It feels worth fighting for, worth suffering for, worth staying for. This is not a delusion or a failure of perception. It is the predictable outcome of a specific set of psychological and neurological processes — processes that operate largely beneath conscious awareness.
🔬 Important Distinction: Trauma bonding is different from simply loving someone who has flaws, or staying in a difficult relationship through loyalty or hope. The defining feature of a trauma bond is the cycle — alternating harm and affection, in a pattern that creates a specific kind of neurological and psychological dependency. If you feel confused about whether what you’re experiencing is a trauma bond, the questions and signs later in this article may help clarify.
How Trauma Bonds Form: The Cycle
Trauma bonds don’t form suddenly. They develop gradually, through a cycle of experiences that — individually — might seem like the normal texture of a complex relationship. It is the pattern, and its repetition, that creates the bond.
The core cycle has four stages, though the labels and pacing vary between relationships:
| Stage | What Happens | What the Bonded Person Experiences |
|---|---|---|
| 1. Harm | Abuse, criticism, rejection, manipulation, neglect, or emotional/physical harm. This may be explosive or subtle — cold withdrawal, contempt, gaslighting, or humiliation. | Fear, shame, confusion, pain, self-doubt. Often accompanied by attempts to understand what went wrong or what they did to cause it. |
| 2. Apology / Reconciliation | The harmful person apologises, expresses remorse, offers explanation, or minimises what happened. May involve promises to change. | Relief, hope, the desire to believe. The apology is emotionally powerful because it resolves the acute distress of the harm stage. |
| 3. Honeymoon / Affection | A period of warmth, affection, attentiveness, and kindness. This may be the version of the person the bonded individual fell in love with — and still loves. | Intense positive emotion, love, relief, confirmation that the relationship is worth it. “This is who they really are.” Neurological reward activation. |
| 4. Tension / Build-up | Mood changes, withdrawal, irritability, criticism, or subtle hostility return. The bonded person senses the shift and often increases their efforts to prevent the next harm phase. | Hypervigilance, walking on eggshells, anxiety, desperate attempts to maintain the honeymoon phase. Return to stage 1 — the cycle begins again. |
What makes this cycle so psychologically binding is not just the alternation of pain and relief — it is the unpredictability of that alternation. The bonded person never knows when the warmth will come or how long it will last. This unpredictability is, as we’ll see in the neuroscience section, precisely what makes the attachment so intense and so difficult to break.
The Childhood Roots of Trauma Bonding
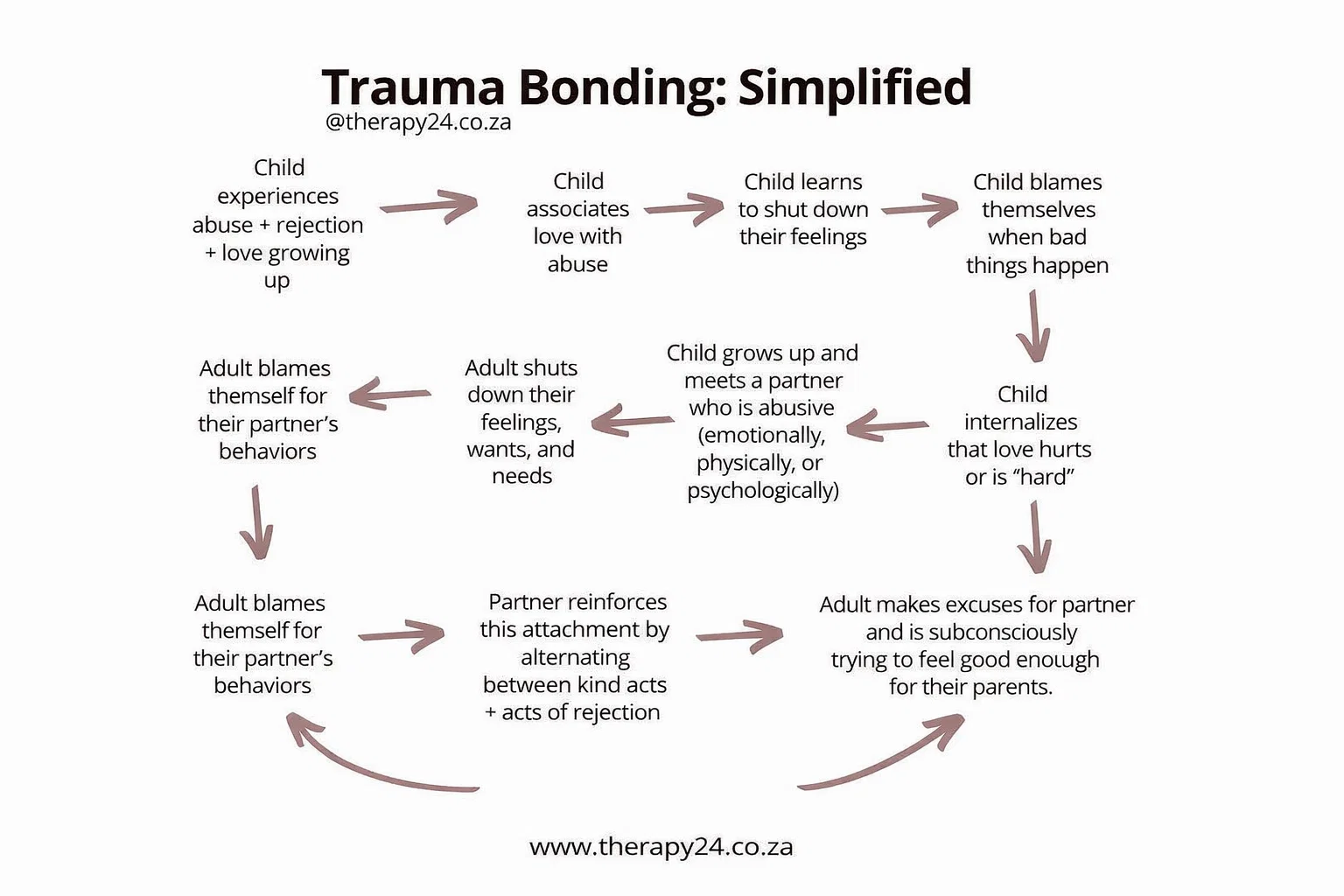
For many people who find themselves in trauma-bonded relationships as adults, the pattern has roots that extend back to childhood — often long before they had the language or awareness to recognise what was happening. The infographic that inspired this article captures this developmental pathway with striking clarity.
When a child grows up in an environment where love and abuse, affection and rejection, are intertwined — when the same person who provides comfort also provides fear — the child’s developing brain and attachment system learn something deeply problematic: that love and pain go together.
This learning is not chosen or conscious. It is carved into the nervous system through repeated experience, at a developmental stage when the brain is maximally plastic and the child is utterly dependent on the caregiver for survival. The lessons learned become the template for what love feels like, what relationships feel like, what “home” feels like.
The developmental pathway often looks like this:
- The child experiences abuse, rejection, or inconsistent love alongside genuine affection from the same caregiver
- The child learns to associate love with the presence of pain — because they have never known one without the other
- To survive emotionally, the child learns to shut down their feelings, needs, and wants — because expressing needs led to punishment or rejection
- When bad things happen, the child blames themselves — “If I were better, more lovable, less needy, this wouldn’t happen” — because self-blame is more bearable than the alternative (that the caregiver is unsafe)
- The child internalises the belief that love is hard, that love hurts, that being loved requires suffering, and that they must earn love by being “good enough”
This child grows into an adult carrying these templates — and when they encounter a partner who alternates between warmth and harm, something deeply familiar activates. Not just familiarity in the sense of recognition, but familiarity in the sense of feeling like home. The chaos, the uncertainty, the intense highs and crushing lows — all of it resonates with the emotional landscape of early childhood, however painful that landscape was.
And unconsciously, the adult relationship becomes an attempt to resolve the unresolved wound of childhood — to finally be good enough, to finally earn the consistent love that was never given, to finally make the relationship work that never worked before.
The Neuroscience: Why Your Brain Stays
One of the most important things to understand about trauma bonding is that it is not a failure of willpower, intelligence, or self-respect. It is a neurological phenomenon — driven by brain mechanisms that are powerful, ancient, and largely outside conscious control.
Intermittent Reinforcement: The Slot Machine Effect
The most important neurological mechanism in trauma bonding is intermittent reinforcement — the same principle that makes gambling addictive. In behavioural psychology, an intermittent reinforcement schedule — where reward is delivered unpredictably, sometimes after a behaviour and sometimes not — produces the most persistent, resistant-to-extinction behaviour patterns observed in any animal.
Slot machines pay out on an intermittent schedule. So do abusive partners. The unpredictable delivery of warmth, affection, and approval — against a backdrop of criticism, rejection, and harm — produces exactly the neurological conditions for compulsive attachment. The bonded person keeps “pulling the lever” — trying, appeasing, being more understanding, being more patient — because sometimes it pays out. And the payouts, precisely because they are unpredictable, are neurologically euphoric.
Dopamine and the Reward System
During the honeymoon phase of the cycle, the brain releases dopamine — the neurotransmitter associated with reward, pleasure, and motivation. But dopamine is not primarily a pleasure chemical — it is an anticipation and seeking chemical. It is released most powerfully not when a reward is delivered consistently, but when it is anticipated and uncertain.
In a trauma-bonded relationship, the bonded person’s dopamine system becomes conditioned to the cycle. The harm phase creates elevated anxiety and craving for relief. When the warmth and affection arrive, the dopamine release is disproportionately intense — far more powerful than it would be in a consistently warm relationship. Over time, the brain begins to require this intensity to feel the sensation of love at all. Stable, consistent love can feel flat or boring by comparison. This is the neurological trap of trauma bonding: the relationship conditions the brain to need the very intensity that harms it.
Cortisol, Stress, and Attachment
The harm phases of the cycle elevate cortisol — the primary stress hormone — and activate the nervous system’s threat response. In a state of elevated cortisol, the attachment system intensifies: the brain drives the person toward proximity with an attachment figure as a source of safety. When the attachment figure is also the source of the threat, this creates a painful paradox — the person is simultaneously frightened of and desperately seeking the same individual. This is the neurological signature of disorganised attachment, which has its roots in childhood experiences of frightening caregivers and becomes the template for trauma-bonded adult relationships.
Oxytocin and Emotional Bonding
Physical affection — touch, sex, closeness — releases oxytocin, sometimes called the “bonding hormone.” Oxytocin deepens emotional attachment and increases trust and feelings of safety. In trauma-bonded relationships, physical intimacy during the honeymoon phase releases oxytocin that deepens the bond — neurologically reinforcing the attachment even when the intellectual understanding of the harm remains fully present. This is one reason why physical intimacy can make leaving harder, even when the cognitive case for leaving is clear.
Signs You May Be Trauma Bonded
Trauma bonding can be difficult to recognise from the inside, because the experience of the bond feels like love — not like a pathological attachment. These signs, taken together, can help identify whether what you’re experiencing may be a trauma bond:
| Sign | What It Looks Like |
|---|---|
| Defending the person who hurts you | You find yourself explaining or justifying their behaviour to others who express concern — “They’ve had a hard life,” “You don’t know them like I do,” “It’s not as bad as it sounds” |
| Minimising or rationalising harm | You downplay incidents that others would identify as clearly harmful — “It wasn’t that bad,” “I provoked it,” “Everyone has their moments” |
| Taking responsibility for their behaviour | You believe that if you were different — more patient, less needy, better in some way — the harm would stop. You are trying to be “good enough” to earn consistent love. |
| Intense fear of losing the relationship | The thought of leaving produces overwhelming panic, grief, or despair — disproportionate to what the relationship is actually giving you |
| Feeling unable to leave despite wanting to | You have left or tried to leave multiple times but returned. The pull back toward the relationship feels stronger than your resolve to leave. |
| Shutting down your own needs | You have learned to minimise, suppress, or feel shame about your own emotional needs — having them seems to cause conflict or rejection |
| The relationship feels more real than others | Stable, kind relationships feel somehow flat, unexciting, or less “real” than the intensity of the harmful one. You may find it difficult to feel attracted to partners who treat you consistently well. |
| Hypervigilance around their moods | You spend significant mental energy reading and monitoring their emotional state — walking on eggshells, adjusting your behaviour to manage their reactions |
If several of these signs resonate, please know: recognising them is not a reason for shame. It is the beginning of understanding — and understanding is the beginning of change.
Where Trauma Bonding Happens
Trauma bonding is most commonly discussed in the context of romantic relationships — but the cycle of harm and intermittent affection that creates it can occur in any relationship where there is a significant power dynamic and repeated exposure to inconsistent treatment:
| Context | How It Manifests |
|---|---|
| Romantic partnerships | The most common context. Cycles of emotional, psychological, or physical abuse alternating with love-bombing, apology, and affection. Can occur in both heterosexual and same-sex relationships. |
| Parent-child relationships | A child’s attachment to an abusive, neglectful, or emotionally inconsistent parent. Because the child is entirely dependent and cannot choose their caregiver, the bond forms regardless of the harm — and often persists well into adulthood. |
| Friendships | Friendships where one person is intermittently warm and then cruel, dismissive, or manipulative. The bonded person may find themselves constantly working to regain the warm version of the friend. |
| Workplaces | Managers or mentors who alternate between recognition and humiliation, praise and criticism. The power imbalance and economic dependency can create bonds that mirror trauma bonding in intimate relationships. |
| Cults and high-control groups | Organisations that use love-bombing during recruitment followed by increasing control, criticism, and conditional acceptance — deliberately deploying the trauma bonding cycle to create loyalty and prevent departure. |
Trauma Bonding Is Not Weakness
This deserves its own section — because one of the most damaging things people tell themselves (and are told by others) about trauma bonding is that it reflects a personal failing. That they should have known better. That they should just leave. That they’re weak, or stupid, or codependent in some shameful way.
None of this is true — and all of it makes healing harder.
Trauma bonding is a survival response. In conditions of threat paired with intermittent warmth, attachment to the source of both threat and comfort is the nervous system’s best available strategy for maintaining safety. It is the same mechanism that kept children alive in difficult family environments for thousands of years of human history. It is neurologically hard-wired, evolutionarily ancient, and activated by specific relational conditions — not by stupidity or weakness.
Research consistently shows that trauma bonding is more common among people who experienced insecure or disorganised attachment in childhood — not because they are broken, but because their attachment systems were shaped by environments where inconsistency was the norm and vigilance was necessary for survival. The adult who cannot leave a harmful relationship is often the child who could not leave a frightening caregiver — and who learned, at the deepest level of their nervous system, that this is what closeness feels like.
Understanding this is not an excuse for staying in a harmful situation. It is the compassion needed to do the work of leaving and healing. You cannot shame someone into breaking a trauma bond. You can only offer understanding — of the mechanism, of the history, of the extraordinary difficulty of the task — and from that understanding, create a path forward.
Healing From a Trauma Bond
Healing from a trauma bond is possible — but it is rarely quick, and it is rarely linear. It requires more than simply ending the relationship. Because the bond is wired into the nervous system, healing is a neurological and psychological process that takes time, support, and intentional work.
Step 1: Awareness — Name What’s Happening
Healing begins with understanding the mechanism. When you recognise that your attachment is being driven by intermittent reinforcement, neurological conditioning, and the echoes of an earlier template — rather than by the inherent worthiness of the relationship — something shifts. The bond doesn’t disappear, but you begin to see it for what it is rather than experiencing it purely from the inside. This cognitive distance is the first handhold on the wall.
Step 2: Reconnect With Your Own Experience
Trauma bonding involves a progressive disconnection from your own needs, feelings, and perceptions — often because those perceptions were repeatedly denied or punished. Healing requires a deliberate process of reconnection. What do you actually feel? What do you actually need? What has happened that was not okay with you? Journalling, therapy, and time spent away from the harmful relationship are all ways to begin hearing your own voice again.
Step 3: Interrupt the Cycle — Create Distance
While the bond remains neurologically active, continued contact with the person maintains and reinforces it. Physical and emotional distance — where safe and possible — is not abandonment of the relationship. It is the prerequisite for being able to see it clearly. This may mean no-contact periods, reduced contact, or — for those in relationships they cannot immediately leave — finding ways to create internal distance through support networks and professional help.
Breaking contact is typically followed by a withdrawal-like period of intense craving, anxiety, and emotional pain — because the dopamine and attachment systems have been conditioned to the cycle. This discomfort is not evidence that leaving was wrong. It is evidence that the bond was real — and that it is beginning to release.
Step 4: Grieve What You Deserved and Didn’t Receive
Part of healing from trauma bonding — particularly when it has childhood roots — involves grieving. Not just the relationship, but what the relationship represented: the hope for consistent love, the belief that this time it would be different, the version of the person you loved in the honeymoon phases. And, for those with childhood roots, the grief for the parent who should have been safe and wasn’t. This grief is not indulgence — it is necessary. Ungrieved wounds do not heal. They go underground and shape future relationships.
Step 5: Professional Support
Trauma bonding — particularly when rooted in childhood attachment disruption — is one of the areas where professional therapeutic support produces the most meaningful outcomes. Several therapeutic approaches are particularly well-evidenced:
- Trauma-focused CBT — addressing the cognitive patterns (self-blame, minimisation, catastrophising about leaving) that maintain the bond
- EMDR (Eye Movement Desensitisation and Reprocessing) — processing the underlying trauma memories that the bond is organised around
- Schema therapy — directly addressing the early maladaptive schemas (deeply held beliefs about self and relationships formed in childhood) that create vulnerability to trauma bonding
- Somatic approaches — working with the nervous system directly, since trauma is stored in the body as much as in the mind
- Attachment-focused therapy — developing a secure attachment experience within the therapeutic relationship that can begin to update the internal working model
Step 6: Build the Evidence That Different Is Possible
One of the most important aspects of long-term healing is accumulating lived experience of relationships that feel different — relationships where consistency is normal, where kindness doesn’t come at the price of fear, where your needs are welcomed rather than punished. This may initially feel unfamiliar, even uncomfortable. The nervous system that learned to associate intensity with love may need time to recalibrate — to learn that calm is not boring, that steadiness is not rejection, that safety is not settling.

What Healthy Love Actually Feels Like
For people who have been trauma bonded — particularly those whose template was shaped in childhood — the characteristics of healthy love can feel foreign or even counterintuitively unappealing at first. Understanding what healthy love actually looks like is part of recalibrating toward it:
| Trauma Bond | Healthy Love |
|---|---|
| Feels urgent, all-consuming, and irreplaceable | Feels secure, grounding, and enriching without being consuming |
| Characterised by intensity, highs and lows, unpredictability | Characterised by consistency, warmth, and emotional safety |
| You feel like you must earn love by being good enough | You feel loved as you are, including in your imperfections |
| Your needs are a source of conflict or shame | Your needs are welcomed and responded to with care |
| You monitor their moods to protect yourself | You feel safe enough to be present rather than hypervigilant |
| Conflict leads to fear of abandonment or punishment | Conflict is navigable and doesn’t threaten the foundation of the relationship |
| You feel smaller, more confused, or less yourself over time | You feel more yourself, more expansive, more capable over time |
Healthy love may initially feel less “exciting” to a nervous system calibrated to the intensity of a trauma bond. But what feels like excitement in a trauma bond is, neurologically, the activation of the threat and craving systems — not the experience of genuine love. Genuine love feels like safety. It feels like being known and welcomed. It feels like being able to breathe. Over time, that safety becomes its own kind of profound — deeper and more sustaining than any intensity could be.
✦ Key Takeaways
- Trauma bonding is a deep emotional attachment that forms in a cycle of harm and intermittent affection. It feels like love — because neurologically, it involves the same brain systems that love activates.
- The cycle — harm, apology, honeymoon, tension — creates attachment through the same mechanism as gambling addiction: intermittent reinforcement, which produces the most persistent and difficult-to-break behavioural patterns in all of psychology.
- For many people, trauma bonding has roots in childhood — in families where love and pain were intertwined, creating a template in which intensity and inconsistency feel like home.
- Trauma bonding is not weakness, stupidity, or a character flaw. It is a neurological survival response to specific relational conditions — driven by dopamine, cortisol, oxytocin, and the attachment system.
- Signs include defending the person who hurts you, minimising harm, taking responsibility for their behaviour, shutting down your own needs, and finding stable love comparatively flat or unappealing.
- Healing requires awareness, distance, grief, reconnection with your own needs and voice, and — for most people — professional therapeutic support.
- Healthy love feels like safety, consistency, and being welcomed as you are — not like urgency, intensity, and the relief of being forgiven for existing.
Frequently Asked Questions
How do I know if I’m trauma bonded or just in love?
The distinction that matters most is the cycle. In a trauma bond, the intensity of your attachment is significantly driven by the relief you feel after periods of harm, withdrawal, or rejection — not primarily by the consistent positive qualities of the person or relationship. Ask yourself: does the love feel most powerful immediately after conflict is resolved, after they’ve been cold and then warm again, after an apology? Do you feel more desperate to hold onto them after they’ve hurt you than you do in the calm periods? If the connection feels most alive in the aftermath of pain, that is a significant indicator of trauma bonding rather than secure love.
Can a trauma bond exist without physical abuse?
Absolutely — and it is important to be clear about this, because many people dismiss their experience because “it wasn’t physical.” Emotional and psychological abuse — contempt, gaslighting, chronic criticism, emotional withdrawal, intermittent rejection, humiliation — can produce trauma bonds as powerful as those formed in physically abusive relationships. The defining feature is the cycle of harm and intermittent affection, not the type of harm. Coercive control, emotional manipulation, and narcissistic relationship patterns all create the conditions for trauma bonding without a single incident of physical violence.
Why do I miss someone who hurt me so much?
Because the bond was neurologically real — regardless of whether the love was healthy. Your dopamine system was conditioned to the cycle of that relationship. Your attachment system is activated. The craving, grief, and longing you feel when separated from someone who harmed you are not evidence that you should return. They are evidence of how powerful the neurological conditioning was — and they are a normal part of the withdrawal process when a trauma bond is being broken. The intensity of the missing typically peaks in the first weeks and gradually diminishes with time and distance, particularly when supported by therapy and connection with others.
Is it possible for the relationship to become healthy?
In rare cases — where both people have deep insight into the pattern, both are committed to genuine change, and both engage seriously with professional therapeutic support — harmful relationships can shift. But this requires the harmful person to take full responsibility for their behaviour without minimising or deflecting, to engage genuinely and consistently with therapeutic work, and to sustain change over a meaningful period of time — not just during honeymoon phases. The probability of this happening without sustained, professional intervention is very low. And it is important to be honest: for many people in trauma-bonded relationships, the hope that the relationship can change becomes part of what keeps them in it — whether that change is likely or not.
How long does it take to heal from a trauma bond?
There is no universal timeline — healing depends on the duration and intensity of the relationship, whether there are childhood roots, the support available, and the therapeutic work done. The acute phase of separation — intense craving, grief, and disorientation — typically diminishes significantly within three to six months of genuine no-contact or distance. Deeper healing of the underlying attachment patterns and self-concept, particularly when there are childhood roots, is a longer process measured in years rather than months. This is not discouraging — it is honest. Deep wounds heal slowly, and that is not a failure.
Can therapy really help with trauma bonding?
Yes — this is one of the areas where therapy has the clearest and most consistent evidence for producing meaningful change. Approaches like EMDR, schema therapy, somatic therapy, and attachment-focused approaches directly address the neurological and psychological mechanisms of trauma bonding — not just the surface relationship patterns. A skilled therapist can help you process the underlying trauma, update the attachment templates formed in childhood, develop a more secure internal relationship with yourself, and build the capacity to recognise and sustain healthy relationships. If cost or access is a barrier, trauma-informed online resources, support groups for survivors of abusive relationships, and sliding-scale therapy options are worth exploring.
🌿 A Note If You’re in This Right Now: If this article has resonated with something you’re living through, please know that what you’re experiencing is real, it makes psychological sense, and you are not alone. Reaching out to a therapist, a trusted person in your life, or a domestic abuse support service in your country is an act of courage — not weakness. You deserve relationships built on safety, consistency, and genuine care. That is not too much to ask for. It is the minimum.
Evidence-based wellness content to help you feel your best — body and mind. | The Whole You Wellness


Leave a Comment